
- This Week in Managed Care: August 6, 2016 (ajmc.com)

Justin Gallagher, associate publisher of The American Journal of Managed Care. Welcome to This Week in Managed Care, From the Managed Markets News Network.
- Drug lobby plans counterattack on prices (politico.com)

Harry and Louise - romancing public opinion
It is just one part of a larger effort by the K Street powerhouse to seize control of the public narrative over drug prices...Washington’s powerful drug lobby is gearing up to spend hundreds of millions of dollars on a post-election ad war pushing back against politicians from both parties who have savaged its members over drug prices...The massive campaign by the Pharmaceutical Research and Manufacturers of America — expected to start positive by highlighting drugs that save or prolong lives — will dwarf the $20 million that health insurers spent on the iconic "Harry and Louise" campaign credited with sinking Hillary Clinton's health reform plan in the early 1990s.
- Rogue online sellers feeding drug abuse (chaindrugreview.com)Internet Drug Outlet Identification Program Progress Report for State and Federal Regulators: July 2016 (s3.amazonaws.com)

Drug abuse, including misuse of prescription drugs, remains at alarmingly high levels...Feeding this epidemic, the National Association of Boards of Pharmacy says, are rogue Internet drug outlets illegally dispensing prescription controlled substances...illicit online drug sellers "hiding behind sleek websites" are making it easier for people struggling with drug abuse to purchase controlled-substance medications. However, since these rogue websites often sell counterfeit and tainted substances, buyers can raise the risk of overdose and death...researchers used popular search engines (Google, Bing and Yahoo), shopping websites (eBay, Craigslist, Yahoo! Shopping, Overstock.com, Etsy, Oodle, eCRATER, Bonanza, Sell.com, Blujay and Alibaba) and social media sites (YouTube and Twitter) to gauge the availability of the opioids Demerol, Dilaudid, Duragesic, Exalgo, Kadian, Lorcet, Lortab, Percocet, Roxicet, Vicodin and Zohydro. Opioids were easiest to find and readily available by using search engines, the researchers discovered. Still, no matter which online avenue was used, researchers found that the final destination was a dedicated website selling opioids illegally.
- Dept of Health to launch sepsis awareness campaign across UK (pmlive.com)

An awareness campaign to improve public recognition of sepsis will be launched across the UK this year, carried out by the Department of Health and Public Health England...Working in collaboration with the UK Sepsis Trust, the initiative aims to better public understanding of the blood poisoning condition that requires quick diagnosis and treatment to effectively combat...Approximately 150,000 adults and children in the UK are affected by sepsis annually, with around 44,000 of those dying each year. If not identified and treated quickly, survivors of sepsis can be left with life-changing disabilities... better sepsis care could save 13,500 lives every year and save the NHS £314m annually...The public awareness drive - called Just ASK: could it be sepsis? - hopes to equip the general public with knowledge of the condition so that they might recognise it and prompt healthcare professionals to fast-track diagnosis of the time-sensitive illness.
- Putting the cost of medicines in context (catalyst.phrma.org)
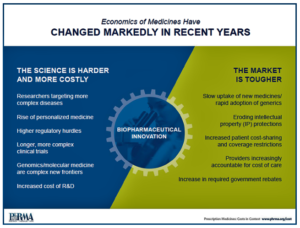
Discussions about costs are important. No patient should have to worry about whether they can afford the care they need. At the same time, it is important to look at costs across the health care system and not just the share going toward life changing medicines...new therapies are transforming care for patients fighting debilitating diseases like cancer, hepatitis C, high cholesterol and more. In the midst of all this progress, the share of spending on retail medicines remains the same as it was 50 years ago. In fact, government actuaries project the share of health care spending attributable to medicines will continue to grow in line with overall health care cost growth for at least the next decade...Our updated Prescription Medicines: Costs in Context explains how competition among brand-name medicines, high generic utilization rates and aggressive tactics by insurers and pharmacy benefit managers to negotiate lower prices all help to keep costs under control...
- Express Scripts bars new launches from Lilly, Merck and shuts out Novo for 2017 (fiercepharma.com)
For the third year in a row, Express Scripts unveiled a new national formulary excluding dozens of drugs. And for the third year in a row, a short list of winners and losers comprises some of Big Pharma’s biggest launches...The list of excluded meds--85 for 2017--covers many of the same brand names as before. For instance, Novo Nordisk’s blockbuster GLP-1 diabetes drug Victoza and two of its top-selling insulins remain barred, as Express Scripts favors Eli Lilly’s diabetes range--and most likely, Lilly’s discounts. AbbVie’s hepatitis C cocktails Viekira Pak and Technivie remain the chosen therapies in that field, with Gilead Sciences' first-to-market meds Harvoni and Sovaldi out in the cold...Express Scripts and its biggest pharmacy benefits rival, CVS Health, started the exclusionary formulary trend a few years ago by kicking off a handful of meds that they saw as too costly and easily replaced...Express Scripts continued its tradition of punishing drugmakers that have pushed through big price hikes, used co-pay discount cards to hawk me-too meds, and employed other strategies the PBM considers no-nos.
- Pharmacy benefit managers are restricting access to lots of drugs next year (statnews.com)The ‘gouge factor’: Big companies want transparency in drug price negotiations (statnews.com)

In the latest bid to control prescription drug spending, the nation’s largest pharmacy benefits managers are again excluding dozens of medicines from their lists of products that are covered by health insurance…Express Scripts notified its customers that next year, 85 medicines will be excluded from its national formulary, and, as a result, the PBM hopes to recognize about $1.8 billion in savings, up from $1.3 billion this year. The number of excluded medicines, by the way, is down slightly from the 88 prescription drugs that were excluded from its 2016 formulary...CVS Health released its own 2017 formulary that will exclude another 35 medicines, including 10 that were called "hyperinflationary." As a result, CVS is now excluding a total of 131 medicines and boasts such moves have saved more than $9 billion over the last five years…Recently, a group of two dozen of the largest names in Corporate America — including Macy’s, Coca-Cola and American Express — formed an alliance (Health Transformation Alliance) to find ways to lower health care costs. One notion they are exploring is to change the way PBMs are paid due to concerns that the rebates the PBMs collect from drug makers on behalf of clients are not always passed along. The PBMs have disputed this argument.
- Pharmacy Week in Review: August 5, 2016 (pharmacytimes.com)

Cate Douglass, PTNN. This weekly video program provides our readers with an in-depth review of the latest news, product approvals, FDA rulings and more.
- Implications of final AMP rule for community Rx (chaindrugreview.com)

On February 1, 2016, the Centers for Medicare & Medicaid Services released its Final Rule interpreting the provisions of the 2010 health care reform law that address the Medicaid Drug Rebate Program. While much of the Final Rule speaks to drug manufacturer rights and responsibilities in the MDRP, significant portions are directly applicable to chain drug stores...the Final Rule addresses (a) reimbursement for multisource drugs dispensed to Medicaid patients, (b) changes in the Average Manufacturer Price (AMP) that will impact pharmacy reimbursement for multisource products, (c) reimbursement for single-source drugs dispensed to Medicaid patients and (d) changes to the dispensing fees pharmacies will receive for dispensing drugs to Medicaid patients...An overarching theme expressed in the Final Rule is CMS’ desire to move states away from their historic practice of overpaying for ingredient cost while simultaneously underpaying for dispensing fees...If the Final Rule plays out as anticipated, in the coming year ingredient cost reimbursement will fall for single- and multiple-source products, but dispensing fees will rise...This reflects a desired shift away from a "spread-based" model of pharmacy Medicaid participation toward a "service-based" model. It’s currently unclear if the increased fee income to pharmacies will balance the lost reimbursement revenue.
- Multisource product ingredient cost reimbursement
- Changes in AMP affecting multisource drug reimbursement
- Single-source product ingredient cost reimbursement
- Medicaid pharmacy dispensing fees
- What Services Should Patients Expect from a Specialty Pharmacy? (specialtypharmacytimes.com)
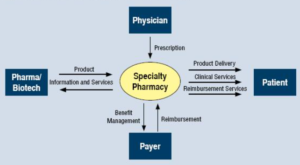
There are 2 important stakeholders when it comes to specialty medications: the patients and the providers. Both groups have a vested interest in the clinical outcome..."what would I expect if I were a specialty patient or a specialized provider?"...Once the reality of the condition begins to set in, then the needed medication must be started to improve clinical outcomes. How would the ideal specialty pharmacy interact with both the patient and their provider?...The ideal specialty pharmacy would have clear upfront communication with both parties. Proactive communication and referral management for the provider would allow the specialist to know precisely what services and capabilities the specialty pharmacy provides...The provider then could inform the newly diagnosed patient that...their expertise, and that of the specialty pharmacy, will ensure the best possible clinical outcomes. At this point, the referral has been sent to the specialty pharmacy, and the patient's interaction with the specialty pharmacy begins.